That's me - Dr Nitin Verma

I'm a Consultant Paediatrician with expertise in Allergy & Respiratory medicine at King's College Hospital London in Marina and Dubai Hills,Dubai (UAE)
I have come to Dubai from the UK, having worked in the NHS for 14 years, last 4 years being a Paediatric Consultant at Darlington Memorial Hospital, UK.
I would endeavour to maintain this blog with the latest available evidence from the medical world of allergy and immunology.
Disclaimer - This is my personal website, and although currently employed at King’s College Hospital London in the UAE, the views and opinions contained within this website may not necessarily reflect the views and opinions of King’s College Hospital London, in whole or in part.
What is food to one is to another bitter poison
Lucretius

Tasty yet a potentially life threatening chalice
Why this blog?
I'm a Paediatrician with expertise in Paediatric Allergy. There is ample evidence available telling us that ALLERGY is a disease/phenomenon (whatever you may prefer to call it) in evolution. I believe its my social responsibility to share my expertise with the wider public. In clinical setting I may be able to reach a few anxious parents/carers/patients whereas with this blog I want to reach out to anyone and everyone who wants to know more about allergy.
What does it mean to have an allergy?
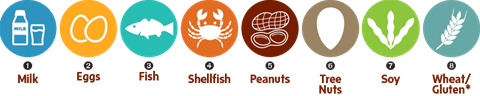
In a child with an allergy, their body triggers an immune reaction each time it comes in contact with a certain allergen which is otherwise tolerated by other individuals . It has to be differentiated from non immune problems like 'lactose intolerance' which is NOT an allergy rather, an enzyme deficiency in the gut .The commonest 8 allergens that trigger an immune reaction are as shown in the picture.
A frequent question that I am asked - how would i know that my child has an allergy? are there different kinds of allergy?
Allergic reactions can be broadly classified into two types:
1) IgE (Immunoglobulin E) mediated - IgE is a molecule in our body that is linked to allergic predisposition of an individual. If for example someone has an allergy to Peanut then in immunological terms it would correlate with an increased level of IgE molecule to Peanut in that individual's body. IgE mediated reactions are the ones that can be life threatening.
IgE mediated allergic reaction generally present within 2 hours of consuming or being exposed to a food allergen and can present in the following ways:
- blotchy red rash (hives) or fine red coloured nettle like rash(pin prick like) that is itchy , anywhere on the body.
- swelling of eyelids, face, lips
- sudden onset sneezing and runny nose
- sudden onset vomiting or diarrhoea with tummy ache
LIFE THREATENING REACTION -
Sudden onset squeaky noise when breathing in (stridor)
Sudden onset breathing difficulty/Wheezing
Tongue swelling
Feeling faint;pale;sweaty;clammy or a collapse
Feeling of 'impending doom' !
2) Non IgE mediated - this is mediated by chemical mediators/cells in our body ( other than IgE). These reactions are generally delayed ( not as sudden as in IgE mediated reactions), even upto a few days after consuming the causal allergen. These reactions predominantly effect the gut and skin. Presenting symptoms are as follows:
- Recurrent episodes of pain abdomen (tummy)
- Recurrent vomiting / loose stools or both.
- Recurrent Eczema flare ups/ Eczema difficult to treat
Toxic reactions (THEY ARE NOT ALLERGIC REACTIONS) to food can occur in any patient, if a sufficient amount of the food is ingested. They are due to toxins in the food, e.g. histamine in scombroid fish or bacterial toxins in food.
What is anaphylaxis ?
Anaphylaxis is a severe allergic reaction (IgE mediated).
It is the extreme end of allergic spectrum where airway, blood pressure or brain is getting effected. the symptoms being:
Swelling of the tongue or throat
Difficulty breathing.
Difficult in swallowing or speaking.
Sudden feeling of impending doom.
Collapse and unconsciousness.
The whole body is affected usually within minutes of exposure to the allergen.
It take seconds to a couple of hours for the symptoms to develop.
What can I do if my child has an allergy?
 pens available")
the 3 adrenaline auto injector (AAI) pens available
AVOID the allergen (if known) . Sometimes its easier said than done but thats the only fool proof way of preventing an allergic reaction.
Try to carry an antihistamine medication with you at all times (Chlorphenamine can be given for children under a year but after that cetirizine (Zirtek®), or loratadine (Clarityn®) is preferable).
In case your child had an anaphylaxis in the past - Please, Please, Please carry 2 Adrenaline auto injector (AAI)pens with you at all times. These AAI pens should be readily accesible whether you are travelling abroad, your child is at nursery, play group, school, sleep over etc.
How to hold an Epipen?
This video describes you the way to grip an adrenaline auto injector pen (Epipen in this case)
There is no video clip yet
Are there any tests to prove that my child has an allergy?

There are 2 common tests that can be performed to figure out whether your child is sensitised to some allergen. These are as follows:
1) Skin Prick Test (SPT) - we place a drop of the relevant allergen on your child’s skin (usually their forearm or upper back). The skin under the drop of allergen is then pricked with a lancet (a metal stick with a small point on the end that scratches the top layer of the skin). By doing this, the allergen gets under the skin surface. We will then wipe away the drop. We can test for several allergens at your appointment. We will repeat the same process for each allergen and make a different mark on your child’s skin with a washable pen for each test. This means we can identify the different allergen tests. After 15 minutes, we will check your child’s skin for a reaction. There are two types of reaction:
- Positive reaction – the skin under the drop of allergen becomes red and itchy. A white, raised swelling called a wheal is surrounded by a red area. This takes about 15 minutes to reach a maximum size and then fades after a few hours. We measure this swelling with a tape measure. If the swelling is above a certain size, this means that your child is likely to be allergic to the substance in the solution.
- Negative reaction – the skin under the drop of allergen remains normal. This means that your child is not likely to be allergic to the substance in the solution.
CAUTION - If your child is taking antihistamine tablets such as chlorphenamine, cetirizine (Zirtek®), or loratadine (Clarityn®), he/she needs to stop taking them at least 4 days before their appointment.
We can perform skin prick tests for a range of foods such as: milk ,egg, soya, multiple nuts, common fish, shell fish, wheat and a range of meat.
We can also test for a wide range of aeroallergens, for example grass and tree pollen, house dust mites, cockroach and pet animals .
If you think your child may have had an allergic reaction to any other food, you can bring a small piece of it with you to the clinic. SPT to fruits is ideally done with a whole piece of the fruit itself.
2) Allergen -Specific IgE blood test -immune system of an allergic person produces antibodies called immunoglobulin E (IgE) to a specific allergen. IgE antibodies are unique to each allergen (for example, IgE produced in response to peanut differs from IgE produced to grass pollen) hence, checking for specific IgE antibodies in the blood can help determine if an allergy is present.
Elevated levels of specific IgE antibodies may mean an allergy is present. However, the amount of IgE doesn't necessarily predict the severity of the reaction. We interpret the results in comparison with your child's symptoms and other allergy tests (SPT).
Comments
Hannah
13.12.2017 08:24
Extremely useful information with so many people now having allergies. This is so important for us all to know what to look for and what to do if we come across someone having a reaction. Thank you!
Ramnik Mathur
12.12.2017 10:27
Excellent website. Loads of useful info. Well done Dr Verma.
mundev rai
23.11.2017 20:41
Definitely needed blog my nephew has a milk n egg allergy, i will signpost him to this blog as its written in a simple easy to understand way...
Cheryl Peart
23.11.2017 11:29
Thanks Nitin very informative both on a professional level and as the mother of a child with a severe allergy.
Arsheena
22.11.2017 08:37
Thanks for sharing this very informative blog Dr Nitin 😊
Jitender Khattar
21.11.2017 02:57
Very nicely written and very informative blog Dr. Nitin I am sharing it with my friend who’s having allergy from green pollen
Saiqa
20.11.2017 23:12
Salaams. Just wanted to ask a quick question... how common is spontaneous urticaria? And does it mean that the person suffering from it can have an allergic reaction to anything?
Jzk.
' fill='rgb(0%2c 0%2c 0)'%3e%3ctitle%3ereply%3c/title%3e%3cpath d='M32 20q0 2.976-2.272 8.064-0.064 0.128-0.192 0.416t-0.224 0.544-0.256 0.384q-0.192 0.32-0.48 0.32t-0.416-0.192-0.16-0.448q0-0.16 0.032-0.48t0.064-0.416q0.096-1.216 0.096-2.208 0-1.792-0.32-3.232t-0.864-2.464-1.44-1.792-1.888-1.248-2.368-0.768-2.752-0.384-3.136-0.096h-4v4.576q0 0.448-0.32 0.8t-0.832 0.352-0.8-0.352l-9.12-9.152q-0.352-0.32-0.352-0.8t0.352-0.8l9.12-9.152q0.352-0.32 0.8-0.32t0.832 0.32 0.32 0.8v4.576h4q12.736 0 15.616 7.2 0.96 2.4 0.96 5.952z'/%3e%3c/svg%3e)
Nitin Verma
21.11.2017 06:06
Hi Saiqa, nearly 30% of all urticarias are idopathic - it means that you cant find any reason for these urticarial reactions despite multiple investigations.i would recommend you see an allergist soon
Dr Turab Syed
20.11.2017 18:51
Thanks Nitin
Andrea Dyne
19.11.2017 23:17
Thanks Nitin, so informative, I’m passing this onto my sister who has a peanut allergy and my daughter who has peanut & multiple allergies so they can both read/share. Good luck with the blog.
Sarah Darwish
Great information, thank you and congratulations on the new blog
Vandana verma
19.11.2017 16:33
19.11.2017 12:53
Very nice read. Looking forward to more.
Seema Sen
19.11.2017 10:10
Really interesting and informative read. Kunal has allergy to Fish but luckily not the IgE mediated type. Look forward to reading further on your blog.
Karen Owens
19.11.2017 09:17
Thanks for sharing Nitin it is definitely something we are seeing more of at Lincoln and is a service we are developing. I look forward to more blogs from you.
Nicola Eeles
19.11.2017 09:16
This is a great idea, very interesting read. Good luck and looking forward in reading more
Lisa Phillips-german
19.11.2017 07:09
Really interesting thank you for sharing look forward to more discussion on topic this is really hard to manage in the wider community unless they have had hospital visit.
Latest comments
13.12 | 08:24
Extremely useful information with so many people now having allergies. This is so important for us all to know what to look for and what to do if we come across someone having a reaction. Thank you!
12.12 | 10:27
Excellent website. Loads of useful info. Well done Dr Verma.
29.11 | 05:00
Brilliant demonstration. Very clearly explained Dr Verma !!! Thanks
23.11 | 20:41
Definitely needed blog my nephew has a milk n egg allergy, i will signpost him to this blog as its written in a simple easy to understand way...
Share this page